
Interferences
Interferences may be present in certain intraoral regions that hinder the easy placement and removal of the prosthesis, thereby affecting the path of insertion.
Several strategies can be employed to manage such interferences:
- Elimination through extraction or surgical intervention,
- Blocking out, filling, or restoration,
- Modifying the design to avoid these regions,
- Utilizing the existing undercut as a retentive advantage.
Soft tissue interferences
Such interferences are commonly observed in the following areas:
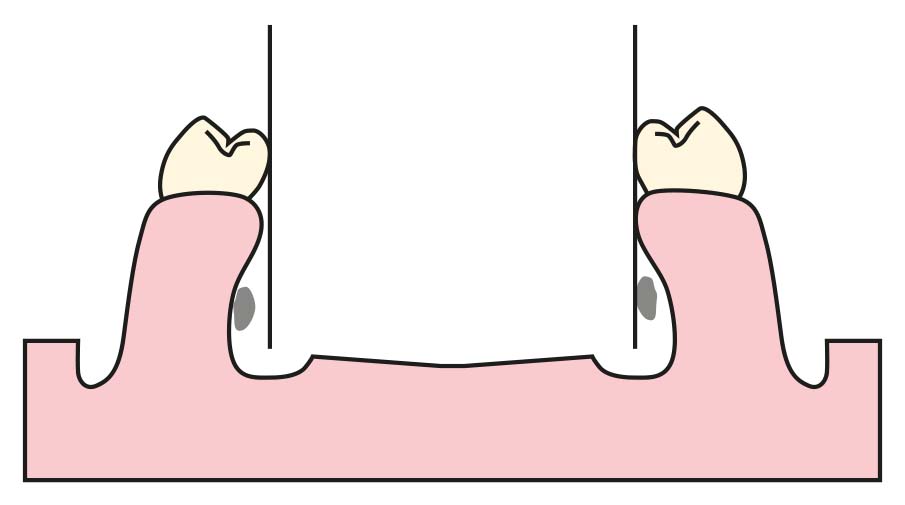
- The mylohyoid ridge, which may become excessively angulated and prominent due to atrophic changes following the extraction of mandibular molars (Figure 7-5),
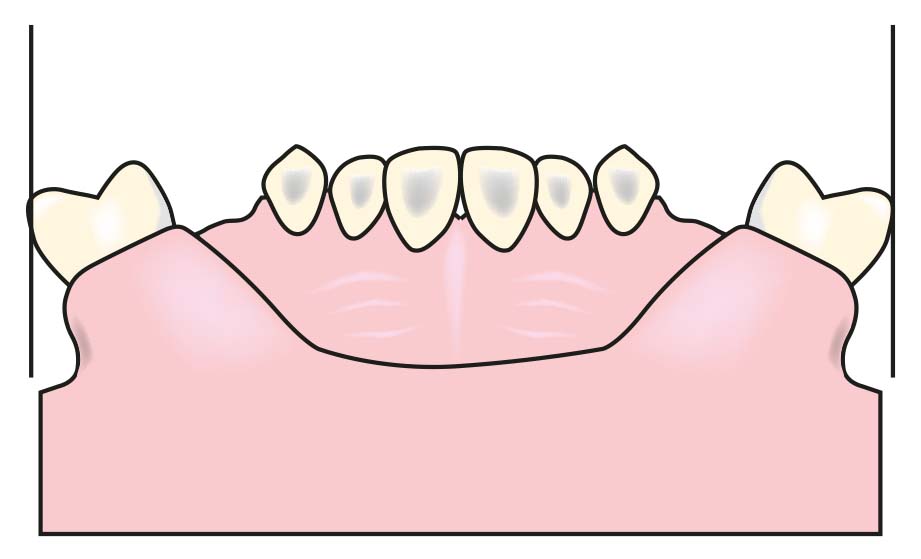
- The tuberosity region, which may become overly prominent either due to its natural anatomy or as a result of lateral expansion of the buccal bone following maxillary molar extractions (Figure 7-6),
- The mental region of the mandible.
These anatomical features should be carefully examined during cast surveying, as they may limit or complicate the intended path of insertion. In general, the bone in the premolar region is not as wide as in the molar region, and it is more tapered in the apical area compared to the crest. In such cases, attention must be paid to adapting the buccal flange of the prosthesis according to the undercut area.


Hard tissue interferences
In both arches, migrated, tilted, or rotated teeth may be present and may interfere with the optimal planning of the prosthesis. These include mandibular teeth inclined lingually or mesially (Figure 7-7), and maxillary premolars and molars that have tilted buccally (Figure 7-8).
Additionally, due to their natural anatomy or atypical positioning within the arch, some teeth may have surfaces that conflict with ideal clasp design.
A commonly encountered issue is that certain abutment teeth have an abnormal height of contour, causing the body and shoulder portions of the clasp to be positioned too close to the occlusal surface. Such tooth contours are typically found at the distobuccal corners of maxillary premolars, the mesiobuccal corners of maxillary molars, and more frequently the mesiolingual, and less frequently the mesiobuccal corners of mandibular molars.
In the mandible, bony prominences in the anterior lingual region and lingually inclined premolars are the main interferences for the placement of a lingual bar.
When these interferences are bilateral, surgical correction or reshaping of the lingual surfaces of the teeth becomes inevitable. However, if the interference is unilateral, tilting the cast “laterally” often provides a solution. Nevertheless, altering the path of insertion to avoid such interferences may result in the loss of the previously determined cast position for guide planes and retentive areas. In such cases, a decision must be made between eliminating the interference or reevaluating the guide planes and retentive areas.
In the presence of bony undercuts, adjusting the lateral tilt of the cast or modifying the design of the denture base—by shortening the buccal, labial, or distolingual flanges—may be considered. However, it should also be kept in mind that maximizing the area covered by the base is important for enhancing denture support.
In the maxilla, interferences that hinder the placement of the major connector are rarely encountered. In cases where posterior teeth are buccally inclined or where bony prominences are present in the buccal region of the edentulous space, it is advisable to first consider modifying the design of the major connector. If this proves ineffective, the path of insertion of the cast may be altered, and the guide planes and retentive areas must be reassessed accordingly.
The surfaces of abutment teeth over which the minor connectors or clasp arms pass must also be evaluated for potential interferences. Although blockout procedures can be used to eliminate interferences for vertical minor connectors, this may cause tongue irritation and food entrapment. Therefore, it is recommended that the vertical arms of minor connectors be used as auxiliary guide planes whenever possible. In cases where significant blockout is required due to an undercut on the abutment tooth, minor changes to the path of insertion or reduction during mouth preparation can be employed to resolve the issue.
The surfaces over which clasp assembly stabilizing arms will pass should also be examined to determine whether there is sufficient space above the survey line. Stabilizing arms placed in the occlusal one-third of the lingual surface of the abutment tooth increase the occlusal dimension of the tooth and, consequently, the occlusal load. Therefore, it is more favorable to position stabilizing arms between the middle and gingival thirds of the lingual surface.
Areas that interfere with the ideal placement of clasp arms are typically managed by reshaping the tooth surfaces during mouth preparation. However, if excessive tooth modification is required, making slight adjustments to the path of insertion or revising the clasp design may be more advantageous.
The most commonly encountered interference areas are the distal corners of the premolar abutments and the mesial corners of the molar abutments. These areas typically conflict with the starting portions of the circumferential clasp arms.
The alternatives to resolve this issue are as follows:
Blockout procedure: This can be performed, but it is not very effective because the clasp’s starting portion is positioned too far from the tooth, which can cause irritation to the tongue and lips and also lead to food accumulation.
Bar clasp arm: The retentive area can be approached from the gingival region using a bar clasp arm. This solution is generally effective when the undercut area on the supporting tooth is not too deep or when there are no soft tissue interferences preventing the placement of the bar clasp arm.
Tooth contour reduction: During mouth preparation, the contour of the tooth can be reduced. If this is necessary, the amount and area to be reduced should be marked with a red pen.
If the undercut area on the abutment tooth is too high or excessively deep, it may still prevent the proper placement of the retentive clasp arm.