
Bar-type clasps
The bar clasp approaches the retentive area of the abutment tooth from the gingival region. The retention created by bar clasps through a pushing mechanism is more effective than the pulling retention of circumferential clasps. Insertion of prostheses with bar clasps is easier compared to circumferential clasps, but their removal is more difficult. Since they approach from the gingiva, they are more aesthetic than circumferential clasps.
The flexibility of the bar clasp can be controlled by the length and thickness of the retentive arm. Increasing its length and tapering towards the terminal end results in a more flexible clasp.
The disadvantages of bar clasps include causing food accumulation and being unable to provide adequate balancing and stabilization due to the excessive flexibility of the retentive arm. When using a bar clasp, additional stabilization elements should be incorporated into the partial denture design.
When a bar clasp extends to the undercut area, it should not cause any trauma to the soft tissues it passes through. Therefore, excessive relief is not recommended, but to prevent trauma, the tissue surface of the clasp arm should be smoothed and polished.
The minor connector attaching the occlusal rest to the framework should be strong and rigid enough to provide balancing.
In distal extension prostheses, the bar clasp is preferred due to its lack of torque effect on the abutment tooth and its aesthetic advantage.
Contraindications for bar clasps:
- Situations requiring excessive horizontal stability.
- Patients with very shallow vestibular spaces that prevent the minor connector supporting the retentive clasp from forming an anatomical relationship with the soft tissue (Figure 3-22a).
- Cases where the minor connector is positioned more than 2-3 mm away from the supporting tissues, leading to soft tissue undercuts or frenulum attachments that cause food accumulation.
- The presence of excessively buccally or lingually tilted teeth that prevent proper placement of the clasp on the abutment tooth (Figure 3-22b).
- Patients with a high smile line, as bar clasps cause an unaesthetic appearance on maxillary canine and premolar teeth.
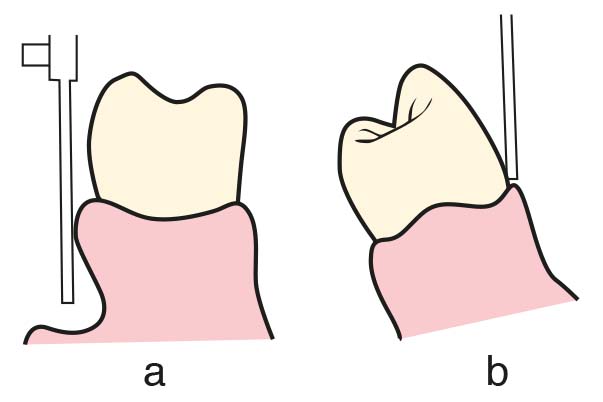
b) Excessive tilting of the supporting tooth towards the lingual or buccal.
Bar clasps can be used on the abutment tooth adjacent to the distal extension base when a small undercut (0.25 mm) is present in the cervical third of the abutment tooth, either in the tooth-supported modification areas or in tooth-supported removable partial dentures. If soft tissue undercuts prevent the application of a bar clasp, a gingival clasp (with horizontally approaching arm) or a reverse Akers clasp may be used.
Bar clasps are typically identified by the shape of the retentive tip, such as T, modified T, I, Y, etc. All of these generally have the same characteristics. As long as the clasp is mechanically and functionally effective, covers as little tooth surface as possible, and minimizes metal visibility, the specific shape of the clasp tip is of no particular importance.
T and Y bar clasp
Since T and Y bar clasps are quite similar to each other, they share common characteristics. Both are frequently used on canine and premolar teeth, and only rarely on molars. This design is particularly useful in distal extension cases where the abutment teeth have distal undercuts. In both T and Y bar clasps, the distal arm terminates within the undercut area, while the mesial arm ends above the height of contour (Figure 3-23).
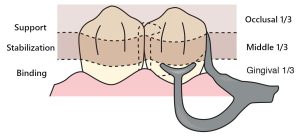
This design not only ensures proper encirclement of the abutment tooth but also contributes to stabilization. When the bar clasp is planned together with a distal occlusal rest, the mesial arm of the T or Y design must be utilized to achieve 180-degree encirclement of the abutment tooth. However, if a mesial occlusal rest is used instead, the encirclement can be accomplished without the mesial arm of the T or Y clasp, and this component may be omitted—resulting in a modified T bar clasp.
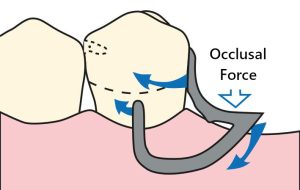
The primary advantage of T and Y bar clasps is that, when the distal extension denture base rotates through mucosally under occlusal forces, the retentive tip of the clasp moves away from the undercut, applying a dislodging force to the abutment tooth that is within physiologic tolerance.
It is unusual for both terminal arms of T and Y bar clasps to be simultaneously positioned in mesial and distal undercut regions. In certain cases, a single arm engaging an undercut may not deliver adequate retention, depending on the anatomical contour of the abutment tooth. When the height of contour is pronounced at both the mesial and distal areas but less prominent in the middle of the facial surface, positioning a Y clasp becomes more practical.
When the height of contour is located near the occlusal surface or incisal edge of the abutment tooth, the use of a T bar clasp is not recommended. Otherwise, a considerable gap may be created between the tooth and the vertical arm of the clasp, leading to food entrapment and irritation of the lip and cheek.
I bar clasp
The I bar clasp is another form of bar-type clasp. It is considered to be more esthetic than T or Y bar clasps or any circumferential clasp, and due to minimal contact with the tooth surface, it is believed to reduce the risk of caries formation beneath the clasp. The I bar clasp is generally used on canines and premolars. Another characteristic of the I bar clasp is its ability to engage an undercut located in the mesiobuccal, distobuccal, or mid-buccal surface (Figure 3-24).
Since the contact area between this clasp and the abutment tooth does not exceed 2–3 mm, it is generally believed that it cannot provide adequate encirclement or horizontal stabilization; however, some researchers argue that the rigid portion of the retentive arm contributes only minimally to stabilization. Due to the limited contact between the retentive element and the tooth surface, special attention must be paid to ensuring the 180-degree encirclement of the abutment tooth, which is a fundamental requirement for all clasps when using an I bar clasp.
RPI clasp
RPI clasp design developed by Kratochvil and Krol, consisting of a mesial rest, a proximal plate, and I-bar clasp, is intended to alleviate the stresses generated by distal extension removable partial dentures. This clasp system essentially consists of a minor connector placed in the mesiolingual embrasure, which does not contact the adjacent tooth, along with a mesio-occlusal rest (Figure 3-25).
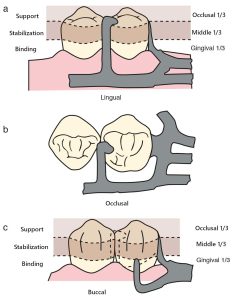
a) Support is provided by the occlusal rest.
b) Stabilization is achieved by the occlusal rest and mesial and distal minor connectors.
c) Retention is provided by the I-bar clasp. Reciprocity occurs due to the positioning of the minor connectors.
To place the distal proximal plate, a distal guide plane is prepared from the marginal ridge extending to the junction of the middle and gingival thirds of the abutment tooth. The buccolingual width of the guide plane is determined by the proximal contour of the abutment tooth. The proximal plate, together with the minor connector supporting the rest, meets the needs of stabilization and reciprocation for the clasp system. The I-bar must be placed in the gingival third of the buccal or labial surface of the abutment tooth, within a 0.25 mm undercut area. The entire approaching arm of the I-bar should be tapered to the point where it contacts the abutment tooth, to a depth of 2 mm, and this taper should not exceed this limit. The approaching arm of the bar clasp should run at least 4 mm away from the gingival margin.
Three principles play a role in the design of the RPI system: (1) the position of the rest, (2) the design of the minor connector (proximal plate) associated with the guide plane, and (3) the position of the retentive clasp arm; these are factors that affect the function of the clasp system.
Changes in these factors will affect the philosophy of the clasp system. All researchers suggest positioning the occlusal rest mesially on the terminal abutment tooth. There are differing opinions regarding the design of the proximal plate. One suggestion is that the guide plane and its associated proximal plate as a minor connector should cover the entire proximal tooth surface, except for a minimum relief that eliminates irritation to the free gingival area. Another approach is that the proximal plate should extend from the marginal ridge to the junction of the middle and gingival thirds of the proximal tooth surface. A third philosophy suggests that the proximal plate should contact the gingival portion of the guide plane at approximately a 1 mm distance.
Gingival clasp
In anterior and premolar teeth, the gingival clasp is preferred when there is a bone and soft tissue undercut in the vestibule of the abutment tooth, which prevents the use of a bar clasp. It is a cast clasp with a retaining arm that runs above the height of contour, with the retentive tip placed in the mesio-buccal undercut. The approach arm is shorter compared to the bar clasp, and instead of running vertically, it extends horizontally parallel to the crest. To allow the clasp to exhibit flexible properties, a modified denture base arrangement should be performed in the region adjacent to the abutment tooth, leaving the approaching arm exposed (Figure 3-26).
