
Denture base
Functions of denture base
Denture base is the part of the prosthesis made of metal and/or acrylic that conforms to the residual ridge and supports the artificial teeth. Positioned to underlie the artificial teeth, it ensures the transmission of occlusal forces to the supporting tissues. Although the primary function of the denture base is to support the artificial teeth, it also contributes to the stabilization and retention of the prosthesis when appropriately designed. Through accurate adaptation of the peripheral flanges, functional shaping of the borders, and intimate contact with the underlying mucosa, it helps counteract stresses caused by tipping and rocking forces acting on the prosthesis. The stabilizing effect of the denture base is often overlooked in clinical evaluations. However, the fundamental planning principle of a removable partial denture base, especially for distal extension cases, is to ensure the widest possible tissue coverage within the limits of anatomical borders and patient tolerance. This allows the distribution of occlusal forces over a broader area, thereby reducing the stress exerted per unit area in a biomechanical context.
Another function of the denture base is to provide stimulation to the tissues overlying the residual ridges through a massaging effect. During functional movements, the vertical displacement of the distal extension base generates stress on the supporting tissues. It has been definitively demonstrated that oral tissues better maintain their form under stress levels within their physiological tolerance limits, and remain in better condition compared to similar tissues that are not subjected to function. The concept of disuse atrophy applies not only to periodontal tissues but also to the tissues of the residual ridges.
In cases of posterior tooth loss, esthetics is generally of secondary concern. However, in the anterior region, where esthetics is of greater importance, the denture base must also fulfill additional roles such as contributing to esthetic outcomes and facilitating the creation of areas that are easy to clean.
While fulfilling these functions, an ideal denture base should also exhibit the following characteristics:
- Good adaptation to the tissues with minimal volumetric change,
- Surfaces capable of forming an ideal finishing line without causing irritation,
- Thermal conductivity,
- Low specific weight,
- Sufficient resistance to fracture or distortion, and
- Compatibility with relining and rebasing procedures.
Types of denture bases
Denture bases differ in terms of their functional purposes:
Tooth-supported denture bases are substructures positioned between two abutment teeth that support the artificial teeth. They transmit occlusal forces directly to the abutment teeth via rests. Both the denture base and the artificial teeth contribute to preventing the horizontal migration of abutment teeth and the vertical overeruption of opposing teeth.
Since tooth-supported denture bases involve abutment teeth at both ends of the edentulous space—each providing support via rests—relining and rebasing procedures are generally not required to maintain support during function. However, relining or rebasing may become necessary in cases of tissue changes leading to esthetic concerns or food entrapment beneath the denture base.
Distal extension denture bases, by contrast, play a direct role in supporting the prosthesis. While the denture have its support with supporting teeth in areas near the primary abutments, the importance of support derived from the underlying residual ridge tissues increases with distance from the abutment tooth. The only way to ensure maximum support from the residual ridge is to fabricate a precise and accurate denture base that distributes the occlusal load evenly across the available tissue-bearing area by using functional impression techniques. To provide maximum support, it is essential to have a thorough understanding of the anatomical structures at the denture borders and the histological characteristics of the underlying tissues, along with obtaining a well-defined impression.
Structurally, a removable partial denture base may be made entirely of acrylic resin, a combination of metal and acrylic resin, or entirely of metal.
An acrylic resin denture base, especially in distal extension removable partial dentures, offers the advantage of being amenable to relining and rebasing after a certain period. A controlled relief is maintained between the base and the tissues over the residual ridge, and the base is connected to the removable prosthesis via a preplanned minor connector (Figure 6-1).

The minor connector is embedded within the acrylic material, which facilitates both the adaptation of the prosthesis and future relining procedures. The thickness of the resin base is also critical in preventing weakening of the resin material surrounding the minor connector, which could otherwise lead to fracture.
The metal-acrylic resin denture base combination consists of a cast metal substructure that conforms to the residual ridge and an acrylic resin superstructure that carries the artificial teeth (Figure 6-1). While it shares both the advantages and disadvantages of a metal base, it is lighter in weight. Since it is not suitable for relining, its use is limited to tooth-supported edentulous spaces.
The metal denture base is often preferred over acrylic resin in tooth-supported removable partial dentures involving short-span edentulous spaces, due to certain advantages. Its stimulatory effect on the supporting tissues helps prevent the alveolar atrophy commonly associated with resin bases, and it maintains the health of the contacting tissues over long periods without undergoing intraoral changes (Figure 6-2).

A metal base does not show surface deformation as a result of functional use since it is resistant to abrasion by surface cleaning products. The self-cleansing properties of metal bases, along with their ability to transmit temperature changes to the underlying tissues, contribute positively to patient acceptance of the prosthesis. However, the major disadvantage of a metal base is the difficulty of relining or rebasing procedures.
In the maxilla, an acrylic base may be preferred over a metal denture base for filling buccal flanges or for esthetic purposes. In such cases, the thinness of the metal base becomes less advantageous, whereas when additional space is needed for the tongue and cheeks, this thin nature may be beneficial. Nonetheless, in terms of shaping the contours necessary for functional contact with the tongue and cheeks, acrylic bases are generally more favorable. Denture bases may be designed entirely of metal, but acrylic resin can be added at the borders to conceal the metal appearance or to provide buccal or lip support where needed.
Denture base design
Due to the structural differences between the upper and lower jaws, the denture bearing area for the prosthesis in the upper jaw is considered to be in a 1.6:1 ratio compared to the lower jaw. Therefore, in order to provide support for the mandibular denture base, the denture border is designed to cover the retromolar pads and buccal plane, in accordance with the principle of covering the maximum area, for distal extension mandibular dentures (Figure 6-3). In cases of bone resorption, these areas will resist changes more effectively compared to the residual ridge region; therefore, prostheses that derive most of their support from these areas will become more stable over time.
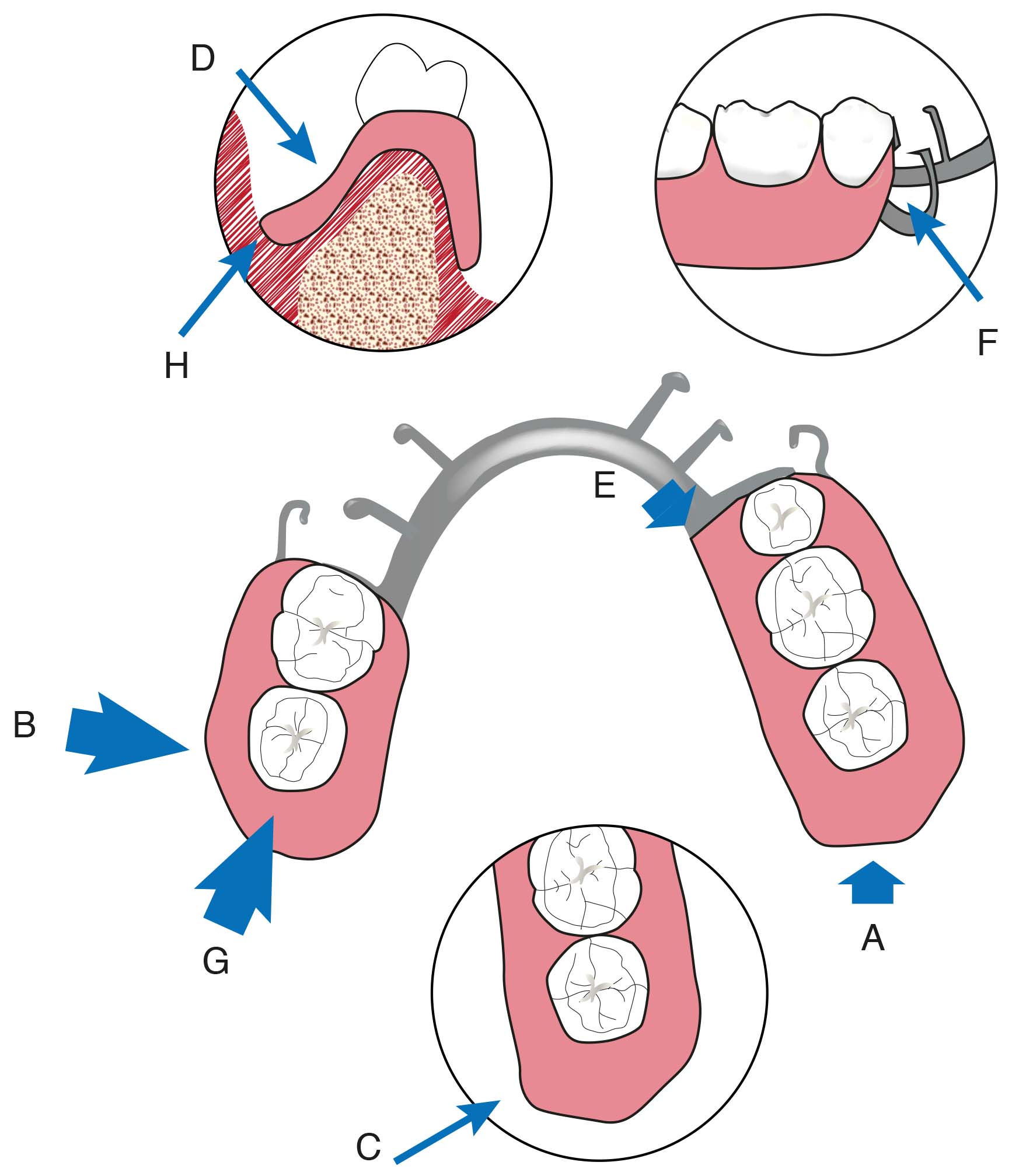
The distolingual border should extend perpendicularly from the apex of the retromolar triangle toward the alveolingual sulcus. Extending the lingual flange beyond the retromolar region does not offer any advantage. The vertical extension of the flange downward depends on the anatomy of the mylohyoid ridge. If this structure is sharp and prominent, the lingual flange may need to be left at the top of this ridge. However, if the mylohyoid ridge is not sharp and does not create a prominent feature beneath it, the flange can be extended toward the alveolingual sulcus to a certain extent. The distal boundary of the lingual flange should curve slightly laterally, and to avoid discomfort to the tongue, the distal edge should be finished with a half-round shape.
The design of the maxillary denture base, on the other hand, is more characteristic of a complete denture (Figure 6-4).
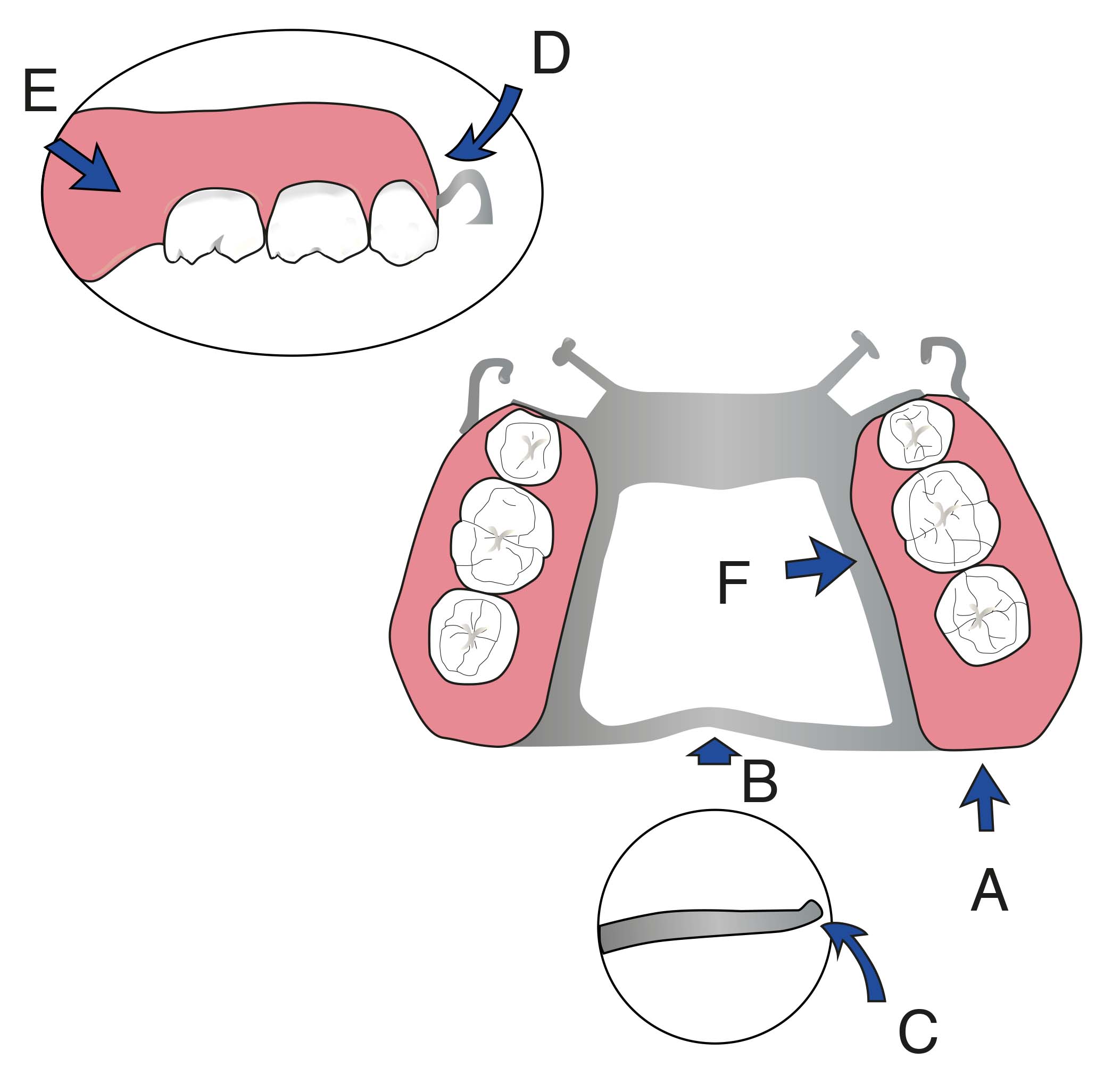
The denture base should cover the tuberosity region and the hamular notch, and the palatal border should be located on resilient, yet stable, tissues. When the denture base includes a buccal flange extending to the premolar region, its anterior part is narrowed toward the posterior region and the borders are thinned. A slightly concave shape is given to the flange to achieve retention through the action of the buccinator muscle. Since the retention of a removable partial denture is primarily provided by natural teeth, the peripheral borders of the base do not need to extend into the vestibular fornix to the same extent as in a complete denture. However, a short base that does not reach the vestibule may result in increased food accumulation beneath it. When an anterior base is necessary, it should be shaped to accommodate the movement of the labial frenulum.