
Chapter 2. Rests and Rest Seats
Providing vertical support in removable partial dentures is of critical importance. The rigid extension of the prosthesis that rests on a tooth or restoration that has been prepared appropriately to provide such support is called a rest. As a controlling component in the denture–tooth–periodontium foundation, a rest might be an auxiliary rest on secondary abutment teeth or a part of a direct retainer.
A rest facilitates the transmission of masticatory forces parallel to the long axis of the tooth when it is placed on a properly prepared rest seat. It also prevents the gingival displacement of the RPD. By maintaining the planned relationship between the tooth and the clasp, the rest ensures the stability of the prosthesis. When positioned correctly, it can function as an indirect retainer. Additionally, it helps to close spaces between teeth, maintains arch continuity, and prevents food impaction. By contributing to a more appropriate occlusal plane, it also prevents the supraeruption of opposing teeth that lack occlusal contact. The primary function of the rest is to control the interaction between the prosthesis and the supporting tissues, thereby providing support for the partial denture.
The most important factor in preserving the supporting tissues is controlling the direction of forces generated during movement and function of RPD. This ensures that the forces are transmitted parallel to the long axis of the tooth and perpendicular to the re-established occlusal plane at the correct position. The key requirement for a rest is to prevent the prosthesis from sliding over the teeth or disrupting the existing relationship between the abutment tooth and the other teeth as occlusal pressure increases. By preventing the prosthesis from embedding and applying pressure on the soft tissues, it also maintains the occlusal relationship.
The rests, which function as supports to keep the partial denture in place, also resist movement in multiple directions. They transfer vertical loads to the abutment teeth and ensure that forces are transmitted along the long axis of the tooth. To effectively perform these functions, the rests must be rigid and receive positive support from the teeth. If they are flexible, the direction of the forces on the abutment teeth may change, potentially causing harm to the supporting tissues. For the rest to establish a continuous and controlled relationship between the tooth, the denture, and the mucosa, it must have adequate size and resistance.
The rests prevent the movement of the prosthesis in the cervical direction and ensure that the retentive tip of the clasp arm remains within the retentive undercut of the abutment tooth. While the tip of the retentive clasp arm remains passive, the other parts of the arm should stay in contact with the tooth. Upon the application of force, the clasp arm becomes immediately active to resist vertical displacement. If the clasp arm moves away from the tooth as the prosthesis is seated, some vertical displacement may occur before the direct retainer becomes functional. The rests contribute to maintaining the stability of the partial denture by preventing impaction.
For the tooth support to be effective, appropriately prepared rest seats on the tooth or restoration surfaces are required. The design and preparation of the rest seat must follow biomechanical principles. This is because the periodontal ligament does not possess cushioning properties, but allows for some compression within the alveolus of the tooth. While all fibers of the periodontal ligament resist vertical stresses, they are less resistant to horizontal stresses. Vertical forces applied to the tooth are transmitted to the bone as “tension” through the periodontal ligament and are relatively well tolerated (Figure 2-1).
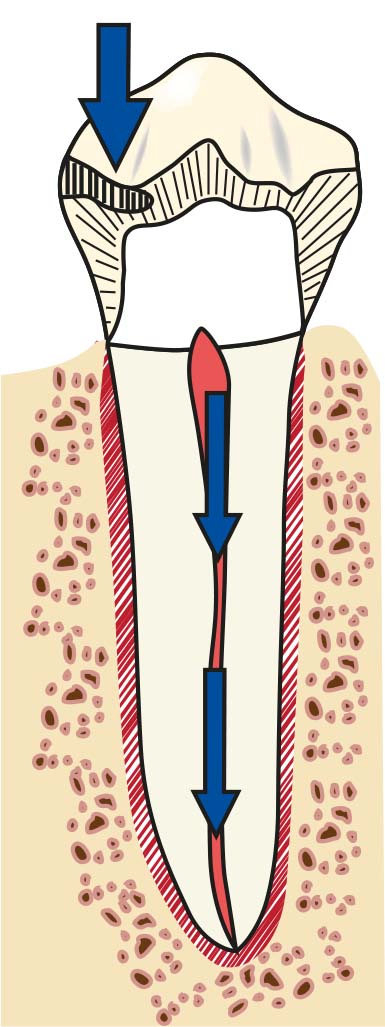
In contrast, horizontal or torsional stresses applied to the tooth are transmitted to the periodontal ligament and bone as “pressure,” which cannot be tolerated (Figure 2-2).
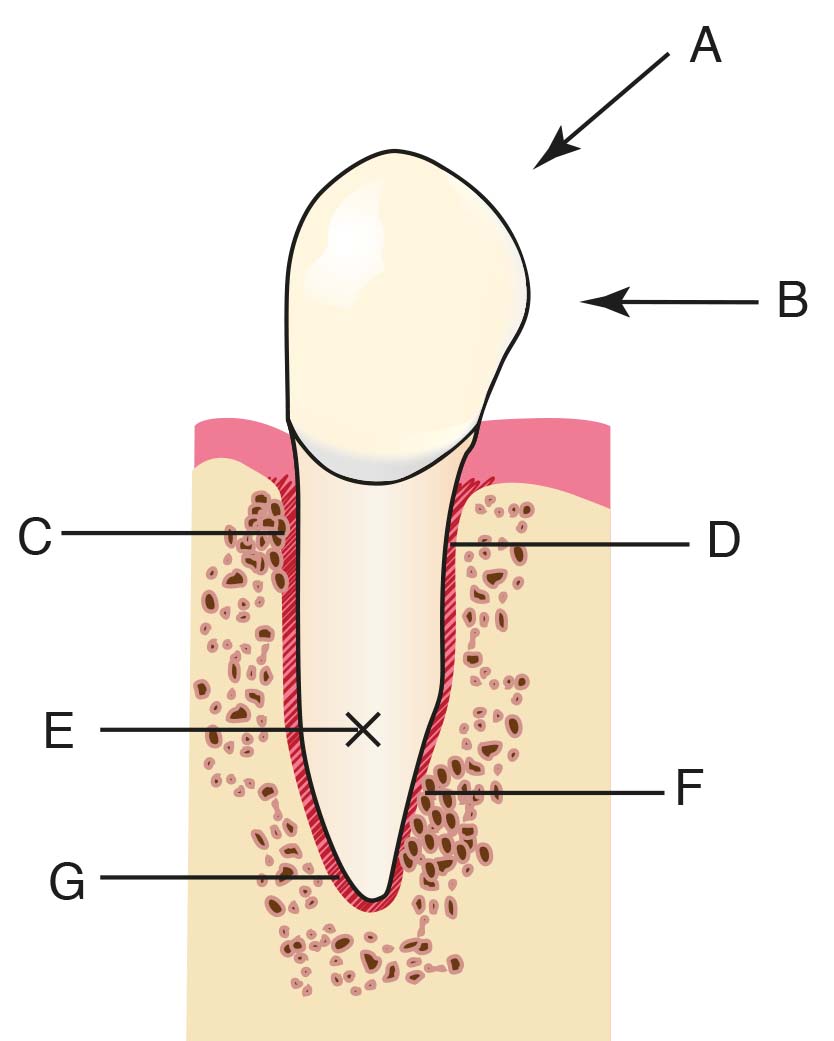
Depending on the magnitude and duration of the stress, damage to the periodontal ligament, even necrosis, and bone resorption may occur. The rest seat should be created at the area of the tooth with the greatest volume, and the force directed toward the tooth should be counteracted by the participation of numerous periodontal ligament fibers. It is equally important to prepare the base of the rest seat perpendicular to the long axis of the tooth in order to reduce torque stresses (See Mouth Preparation; Chapter 10).
Vertical support is provided from the widest part of the tooth (contour height), from the occlusal surface, or sometimes from the inclined tooth surfaces at the incisal. According to these regions, the rests are categorized into three groups:
- Occlusal
- Lingual (singulum)
- Incisal