
Chapter 9. Occlusal Relationships for Removable Partial Dentures
Occlusal harmony between the removable partial denture and the remaining teeth is a key factor in maintaining the health of surrounding tissues. In RPD cases, the number and position of the remaining teeth determine the occlusion. The type of occlusion is clinically analyzed based on contacts during mandibular eccentric movements. The stability of the RPD must be maintained in both centric and eccentric contacts.
The following considerations are important in establishing occlusion for RPD patients:
- Analysis of existing occlusion
- Correction of occlusal disharmony
- Recording of centric relation
Analysis of existing occlusion
The primary principle in all occlusion types is to achieve maximum contact between the opposing cusps and fossae during centric occlusion. Lateral movements determine the type of occlusion.
The patient’s lateral mandibular movements (right and left lateral excursions) are evaluated, and the existing occlusion is identified based on the contacts of antagonist teeth on the working and non-working sides during these movements.
The lower canine’s incisal edge remains in contact with the upper canine’s palatal surface while the mandible moves laterally. If the incisal edge of the lower canine makes contact with the incisal edge of the upper canine after the lateral movement completes and disclusion (absence of contact) occurs on the other opposing teeth, the patient’s current occlusion is known as canine-guided occlusion (Figure 9-1).

During lateral movement, if the premolars contact along with the canine on the working side, it is defined as group function occlusion; if one or two molars as well as posterior teeth are in contact on working side, it is called unilateral balanced occlusion (Figure 9-2).

In canine-guided, group function, or unilateral balanced occlusion, only working contacts need to be formulated. For example, during right lateral movement, there is no contact between the opposing teeth on the left side. In lateral movements, only the antagonist teeth on the working side toward which the movement occurs make contact. In protrusive movement, antagonist contact occurs between the anterior teeth, while disclusion is present in the posterior region.
In cases where there are no antagonist tooth contacts, the patient’s occlusion is re-established based on the condition of the partial edentulism and according to the criteria outlined below. One such occlusion type—bilateral balanced occlusion—is typically applicable in these cases.
As with other occlusion types, simultaneous bilateral contacts of opposing posterior teeth must occur in centric occlusion in bilateral balanced occlusion (Figure 9-3).

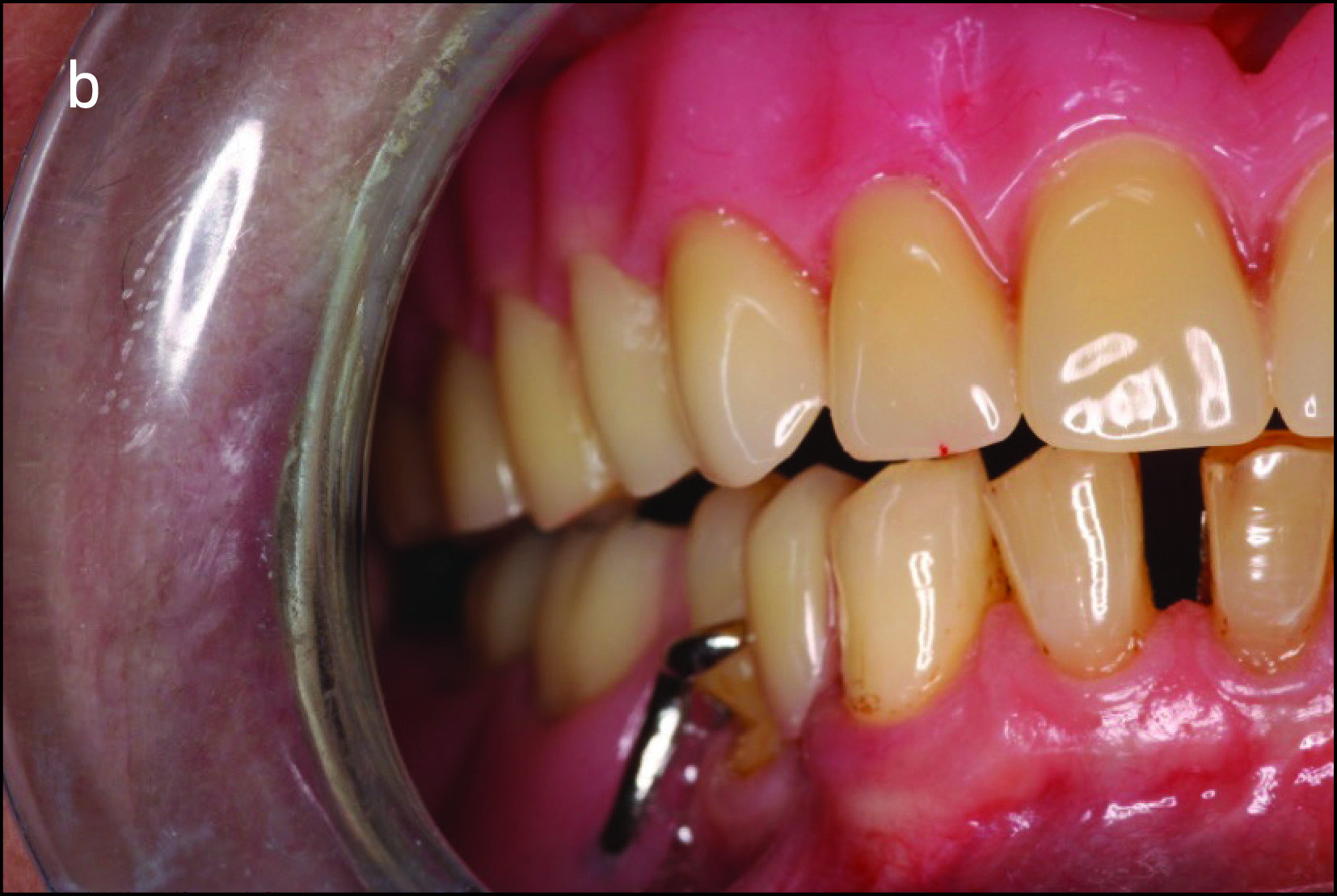
In bilateral balanced occlusion, during lateral movement, there are simultaneous bilateral contacts of opposing posterior teeth on both the working and balancing sides. For example, during a left lateral movement, antagonist tooth contacts occur on the working side primarily through the buccal cusps in the posterior region (Figure 9-4a), while on the opposite side, the buccal cusps of the mandibular teeth are in contact with the palatal cusps of the maxillary teeth. This prevents the right side of the removable prosthesis from lifting off the tissue (Figure 9-4b).

In protrusive movement, the incisor teeth are in an edge-to-edge position in the anterior region, while simultaneous contacts are established between the second molars on both sides in the posterior region, creating a “three-point contact.” This prevents the posterior denture bases from lifting off the tissue during anterior biting movements (Figure 9-5).

However, in order to achieve proper protrusive contact, the overbite distance should not exceed 1 mm. In such cases, the incisal edges of the upper anterior teeth may not be visible during smiling, and the attempt to ensure protrusive balance may compromise esthetics. Therefore, the patient’s opinion must be considered, and it should be acknowledged that establishing protrusive balance may be difficult in patients who prioritize esthetics. Such patients should be advised to avoid anterior biting movements. Conversely, for patients who prioritize biting function, they must be informed that the visibility of their teeth during smiling may be reduced. In this situation, the patient will have to choose between using the anterior teeth for incising or achieving an esthetically pleasing appearance.
Correction of occlusal disharmony
Occlusal discrepancies negatively affect the success of the prosthesis. In partially edentulous cases, due to reasons such as loss of teeth at different times or prolonged edentulism, the remaining teeth tend to tip, drift, or supra-erupt into the edentulous spaces (Figure 9-6).

Teeth can occasionally remain in their proper places, in which case the patient should be commended for their good fortune. Enameloplasty, or enamel-level reshaping, may be adequate if elongation or tilting is minimal; in more severe situations, crown restorations would be necessary. To adjust the occlusal plane level, however, root canal therapy may typically be required prior to crown restoration. In more severe cases—such as when a tooth has elongated to the point of contacting the opposing ridge—extraction may be considered due to the accompanying loss of periodontal support. The most appropriate course of action should be determined using diagnostic casts on which accurate occlusal relationships have been established.
Recording of centric relation
The method used for recording centric relation is determined by the class of edentulism and the presence of antagonist tooth contacts.
When there is sufficient antagonist dentition, models are brought together directly in tooth-supported cases.
When there are insufficient antagonist teeth, interocclusal registration materials are used to articulate the models.
In cases where the opposing arch has a complete denture and there are distal extension areas or no antagonist tooth contacts, record bases and occlusion rims are utilized.